The media headlines have been everywhere, but the truth is we know very little.
Like everyone here, I was surprised at the *universal* instant Omicron media coverage which went from 0 – 100 in two seconds or less. I’m going to skip (for the moment) the obvious political questions like “is this the midterm election variant” and consider the virus.
…
We know Omicron has many mutations. We don’t know what the combined effect of them is. Presumably the particular mutations, and lab tests of antibody binding suggest it may evade vaccine or even natural immunity. However, many of these mutations are new and unknown, so the in vivo, real effect is only something the patients and doctors might know. And the doctors are giving mixed reports in South Africa. It may turn out to be a more infectious but nicer variant. We’ll know in a few weeks.
It’s certainly spreading fast. Case numbers have increased six-fold from 300 cases to 1,800 in just two weeks. Test numbers are up but test positivity has also risen from 1% to 3.7%.
Symptoms have changed. Doctors say that they noticed a change in the presentation of cases around 10 days ago. The symptoms were suddenly different, and while Dr Angelique Coetzee, said it appeared to be mild, (which is very encouraging) she was referring to young patients, and is still concerned about older patients. The new symptom list includes headaches, extreme tiredness, body aches and pains, but not a loss of smell, or coughing.
But Rudo Mathivha, head of Soweto’s Baragwanath hospital said that young people in their 20s to 30s are coming in with moderate to severe disease, some needing ICU. That’s not good.
About 65% are not vaccinated. John Campbell interprets this to suggest that the unvaccinated are at higher risk, but if only a quarter of South Africans are double vaccinated, and the vaccines work, shouldn’t we see even more unvaccinated patients than that? Wouldn’t most of the young people be unvaccinated?
Omicron has already been circulating somewhere for more than a year
Looking at the evolutionary history of these mutations — the last and nearest branch was around May 2020. That means it’s likely that the Omicron variant has been silently spreading in a population that is rarely if ever tested or sequenced. That would explain why so many mutations seem to have “suddenly” appeared. Presumably if it was a variant that was very deadly, it would have come to our attention months ago, even in a remote African village, surely? Though if it has been circulating in Africa (and we don’t know that) it has probably been affecting a younger population, possibly one that’s fitter or leaner and which gets more sun (and Vitamin D). We don’t know the effect it has on the older, indoor, and more diabetic people of The West, and we don’t know much about the effect on people who are vaccinated, either. Assume that it has become more infectious recently, but collecting mutation for a long while.
It may be a blessing that this variant has evolved in a region that has low vaccination. It might be less deadly. But we don’t know that, yet. It’s possible that even a virus that is milder, but spreads much faster will ultimately cause higher mortality. (Think of SARS-2, compared to SARS-1). But the new variant might be good news. What we want, after all, is for it to evolve into a highly infectious mild disease.
The solution is still antivirals and borders (til we get antivirals)
The key to this is still antivirals. Because Ivermectin has so many mechanisms of action, many that apply to our own molecules (ACE2, TMPRSS2, Ribosomes, Importin) even if ivermectin didn’t bind to the new Omicron spike, it would still be very useful against the virus. So start right now. It should be offered to people at risk.
Given the risk of Antibody Dependent Enhancement (ADE) in vaccinated people, and the risk it might pose to unvaccinated seniors and the co-morbid, it makes sense to shut borders for a couple of weeks, just to get more information. Though possibly it’s already too late, since the virus has been found in so many places. And if reports that Dutch Authorities detected Covid cases in 61 out of 600 passengers from South Africa on Friday morning are true, and those passengers are also vaccinated, wow? Did they catch it on the flight? Update: Apparently only 13 of the 61 cases were the Omicron variant.
The value of a travel ban is the time it gives to test the antivirals in the lab, test the virus against the antibodies, test the virus against the tests! How many cases are we missing?
Of course, it makes no sense to tell everyone that vaccines are the solution to a variant that might be able to escape vaccines. Not coincidentally, Big Pharma is suddenly saying they can develop a new vaccine pronto, which is why they were so keen on using the experimental mRNA vaccines in the first place. But we still have no long term data and much better alternatives.
Omicron has probably been circulating for a long time
In order to collect so many mutations and to have been undetected for so long, it’s likely this branch of the virus was wandering through a population that rarely gets tested. Presumably, they are also rarely vaccinated. This may turn out to be a good thing.
The new Omicron branch is marked in red below.
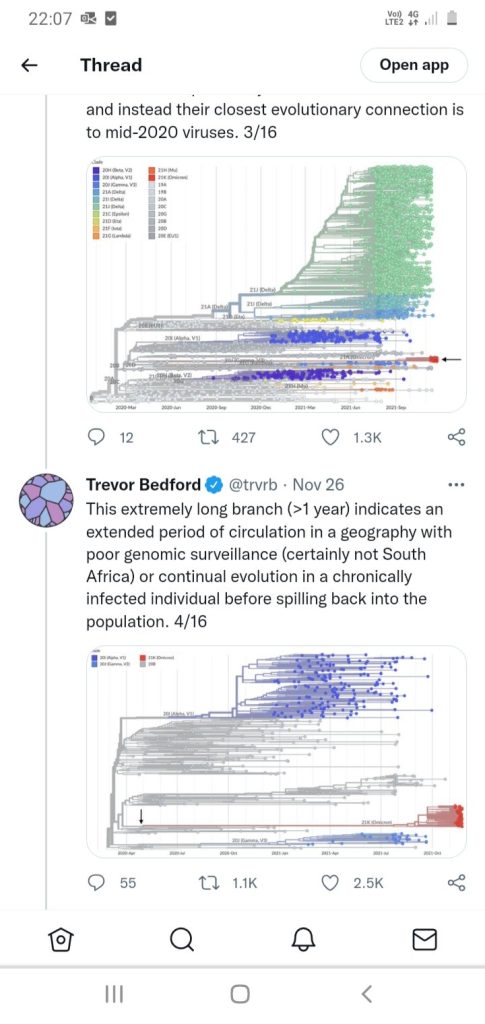
Omicron has probably been roaming for a year undetected. The last branch, marked with a black arrow dates back to May 2020.
Either that, or Omicron is an artificial variant, planted from somewhere. Who knows? It’s theoretically possible for a malicious gene lab to take a sample, add some tweaks, and drop it anywhere. We need mass testing to find the missing links to be able to say whether this is absolutely a natural infection branch, and find where it has been hiding.
It’s spreading fast
Cases have increased about six-fold in the last two weeks from around 300 to 1,800. Source: OWID
South Africa has had three waves. Source: OWID,
Omicron has rapidly overtaken Delta in South Africa, but this was during a time when cases were very low, so the sample size for the mass Global Headlines is surprisingly and suspiciously small (the trend line is heavily dependent on just a few cases).
For perspective, when Delta surged and overtook in May 2021 there were 400-800 samples on the graph in South Africa, but the current total tally on Nextstrain used to generate this “prevalence” graph was only 6 cases. (Mouseover the graph on the source page to see case numbers.) Perhaps there are many more samples that haven’t been reported to the Nextstrain database?
Obviously the trend of “rapid” growth is there, but the number of samples is small. Source: Nextstrain
Omicron has a lot of mutations
Many of these also occur in other strains and have been studied (top half). But many are new (bottom half). We really have no idea what effect the latter have. It may be nothing, or everything.
Omicron contains man shared mutations (top), but also many new ones (lower half). Source: Nextstrain.