How many unnecessary deaths does it take til people get angry? Angry that the Chief Medical Officers and Health Ministers didn’t ask for studies to be done. Angry that most academics sat by and said nothing. And angry that the media just parroted the institutions.
One good antiviral changes everything. If the world had a safe cheap drug, we could not only reduce deaths and disability, but also slow the rate of mutation down and probably slow the appearance of new mutations down.

…
The Chamie-Quintero study from Peru shows the West could be only weeks away from reducing the Covid death toll if we used the safe cheap sheep-dip, lice-killing Ivermectin like less wealthy countries do.
A study across the states of Peru found that after Ivermectin was introduced, deaths started to fall about 11 days later, and within a month after that, deaths were down around 75%.
Ivermectin is a drug so useful early researchers got a Nobel Prize in Medicine for work on it. It’s so well known that in the last thirty years more than 3.7 billion doses of Ivermectin have been given out. It’s so safe we can use it on cats and dogs and even toddlers. It’s dirt cheap and its use in Ag-science is measured in tonnes. The cost of Ivermectin is around 15c in the third world, and $50 for one round for a human in New York. (It’s a lot cheaper than a $5000 a day ICU bed.)
Ivermectin first showed promise against Covid in a lab dish back in April. It wasn’t clear if it would work as well in people, but it was so cheap and safe that the rich world …o, pretended it didn’t exist and tested expensive drugs instead. (Big-Pharma don’t make big profits from old cheap drugs that are out of patent.) Meanwhile less wealthy countries were desperate enough to try it en masse. And Ivermectin has had remarkable success.
Something like 3 out of 4 people who were on the road to dying appear to have been saved.
“… excess deaths at +30 days dropped by a population-weighted mean of 74%.
But this is not a neatly controlled experiment. The mortality curves may have declined anyway for other reasons. But then there is this:
…each drop beginning within 11 day after MOT start” (MOT stands for Mega-Operación Tayta.)
Bear in mind that this doesn’t mean Ivermectin will save 74% of people who are already sick. The lags in this study suggest it partly works to limit the spread of the disease. People with less virus, may shed less, die less and not infect so many other people.
It shows what doctors can do: Ivermectin was already nationally approved in Peru by May 8th and it was rolled out across the nation between April to August. As is the way, the last people in Peru to get easy access were the unfortunates in the the Capital city Lima. Things were delayed there by four months by some strange practices like “restrictive measures on IVM distribution, including police raids on pharmacies.” Thank Big Gov.
Such was the severity of the pandemic that in May excess deaths in Peru were running at twice the mortality they ran in January and February (in winter, doh, summer).
Each line below is a state of Peru and they are all lined up at day 0 – which was the peak day of deaths — the day the inexorable rise suddenly ended. The only state without a rapid decline was Lima (red) which didn’t get Ivermectin til four to five months after most other states. By which time people had quite possibly been smuggling Ivermectin into Lima, smoothing the curve out.
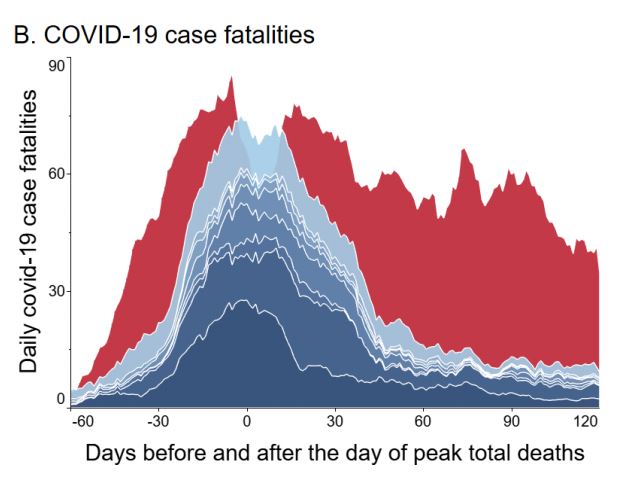
B) COVID-19 case fatalities tail off quickly everywhere except Lima (red).
The tell-tale lag pattern
The pattern keeps repeating. Death are rising. Ivermectin starts and within 11 days deaths start to fall.
I. D) Excess deaths for nine states having mass IVM
distributions in a short period through national operation “MOT” (see results section for sources). ● MOT start date; ▲peak deaths; ■ day of peak deaths + 30 days. Junin (yellow) distributed IVM to health centers beginning on July 22, 13 days before MOT start. Population-weighted mean deaths for these nine states dropped sharply, -74% at +30 days, beginning (except for Junin) 1 to 11 days after MOT start. All y values are 7-day moving averages, ages ≥ 60.
At a higher dose Ivermectin may be 90% effective:
Doses in Peru were quite low, and Ivermectin may save even more lives at a higher dose.Get a load of these numbers:
Since the May 8 authorization in Peru, 11 clinical trials of IVM for COVID-19 treatment,12,16-25 three of these with randomized controls,17,19,20 have shown major reductions in mortality and severity. Mortality rates for IVM treatment at higher doses, totaling at least 400 μg/kg over two consecutive days, were about one-tenth those of controls, with statistically significant improvement in other case parameters.17-19 In a randomized controlled trial for IVM prophylaxis, a group of 203 household contacts of COVID-19 cases given IVM had one-eighth the COVID-19 incidence (7.4% vs. 58.4%) and one-fourteenth the severe case incidence (0.5% vs. 6.9%) of the control group.26
Only the late Lima (red) has a different pattern to the other states. The excess deaths pattern suggests Lima’s first outbreak was the worst, especially when the testing was so inadequate.
Figure 1: Graphical Abstract. A) Excess all-cause deaths
The falling death rates were not due to changes in the virus, herd immunity or population density:
Researchers wondered if the virus might have rvolved to have been nastier in Lima, but genetic studies showed there were similar strains. Researchers thought herd immunity might have been responsible but the antibodies studies suggested only 20% of the population had immunity. And the reduction in fatalities was just as large in areas with more immunity. And population density didn’t explain it either. Lima is the most densely populated but other places still have 80 – 90% of the density. One researcher though that people who had survived dengue fever had some protection from Covid, because that pattern looked real in Brazil. In Peru, that was not the case.
Herd immunity was probably not the reason the deaths reduced:
The possibility that the development of herd immunity was responsible for the observed reductions in mortality in the 24 states with early IVM treatment but not Lima is discounted by consideration of stateby-state seropositivity rates for November 2020 (Table S6). Although a high seropositivity rate for Loreto, which had reached 75% even by September, 99 could explain reduced pandemic impacts there, several other IVM-treated states with low seropositivity rates had sharp drops in COVID-19 mortality. For Cajamarca, Cusco, Huancavelica and Tacna for example, all having IVM distributions through operation MOT, seropositivity rates even with increases through November were only 20%, 18%, 18%, and 15%, respectively. But within 1 to 8 days after MOT start, excess deaths peaked and then dropped over 30 days, respectively, by 63%, 86%, 75% and 81%. For Arequipa, Amazonas and Ucayali, to cite other examples of states deploying IVM treatment, seropositivity rates in November were 20%, 26% and 40%, but reductions in excess deaths 30 days after peak deaths were 65%, 84%, and 87%.
Ivermectin is a prescription drug in most countries. As with all drugs there are risks. Other infections, parasites and unlucky gene combinations can be deadly. Doctors have a very good idea of who is at risk.
h.t David Archibald. Old Ozzie, Hanrahan, David Maddison. Furiously Curious. Gregg, Lance, Craig Kelly MP!
REFERENCE
Chamie-Quintero, Juan and Hibberd, Jennifer and Scheim, David, Sharp Reductions in COVID-19 Case Fatalities and Excess Deaths in Peru in Close Time Conjunction, State-By-State, with Ivermectin Treatments (January 12, 2021). Available at SSRN: https://ssrn.com/abstract=3765018 or http://dx.doi.org/10.2139/ssrn.3765018